 Incorect Politic O Publicație Dizidentă
Incorect Politic O Publicație Dizidentă
Sterie Ciumetti
Incorect Politic
Noiembrie 11, 2020
Avem cel mai complex studiu științific care demonstrează fără drept de apel că măștile nu doar că sunt ineficiente, dar sunt și dăunătoare. Este un material amplu, de specialitate, pe care îl reproducem integral, în limba engleză:
https://www.meehanmd.com/blog/2020-10-10-an-evidence-based-scientific-analysis-of-why-masks-are-ineffective-unnecessary-and-harmful/
About Dr. Meehan
Jim Meehan, MD is an ophthalmologist and preventive medicine specialist with over 20 years of experience and advanced training in immunology, inflammation, and infectious disease. He has performed well over 10,000 surgical procedures. His research experience includes investigating associations between military vaccinations and Gulf War Syndrome. Dr. Meehan is also trained in internal medicine, addiction medicine, endocrinology, integrative medicine, functional medicine, and nutrition.
Dr. Meehan is a former editor of the medical journal, “Ocular Immunology and Inflammation.” Dr. Meehan has peer-reviewed thousands of medical research studies. With this experience and expertise, Dr. Meehan has dedicated his career to protecting his patients and the public from the fraud, corruption, and pseudoscience so often used by agents and agencies whose motives and interests have resulted in American medicine and pharmaceutical drugs becoming the third leading cause of death in the United States.
Key Points
- Decades of the highest-level scientific evidence (meta-analyses of multiple randomized controlled trials) overwhelmingly conclude that medical masks are ineffective at preventing the transmission of respiratory viruses, including SAR-CoV-2.
- Those arguing for masks are relying on low-level evidence (observational retrospective trials and mechanistic theories), none of which are powered to counter the evidence, arguments, and risks of mask mandates.
- The majority of the population is at very low to almost no risk of severe or lethal disease from CoVID-19. Children are at an extraordinarily low risk of dying from CoVID-19. Based on CDC published data, 99.99815% of children that contract CoVID-19 survive.
- Transmission of SARS-CoV-2 among children in schools and daycares is very rare.
- Masks worn properly are well documented to cause harm to their wearers. Masks worn improperly, re-used, or contaminated are dangerous.
- Any reasonable risk to benefit analysis of medical masks concludes that the risks overwhelmingly outweigh the benefits.
- Children are at imminent risk of harm from mask mandates.
Outline
- Evidence Based Medicine: How we (should) make decisions in science and medicine
- Masks are Ineffectivea. Mixed Messages from the Expertsb. The Evidence Against Masks
c. The Evidence For Masks
- Masks are Unnecessarya. Fear and Politics are Subverting Science and Reasonb. Masking Children in Schools is Unnecessary – So Says The Science
- Masks are Harmful: 17 Ways that Masks Can Cause Harm
- Masking School Children is Ineffective, Unnecessary, and Harmfula. Mandatory masks in school are a ‘major threat’ to children’s’ health, doctors warnb. Forcing Children to Wear Masks in Schools is Unnecessary
c. Forcing Children to Wear Masks for Long Periods Risks Causing Them Physical Harm
d. Forcing Children to Wear Masks for Long Periods Risks Causing Them Mental and Psychological Harm
Evidence Based Medicine: How we (should) make decisions in science and medicine
High-level versus Low-level Evidence – the Hierarchy of Medical Evidence
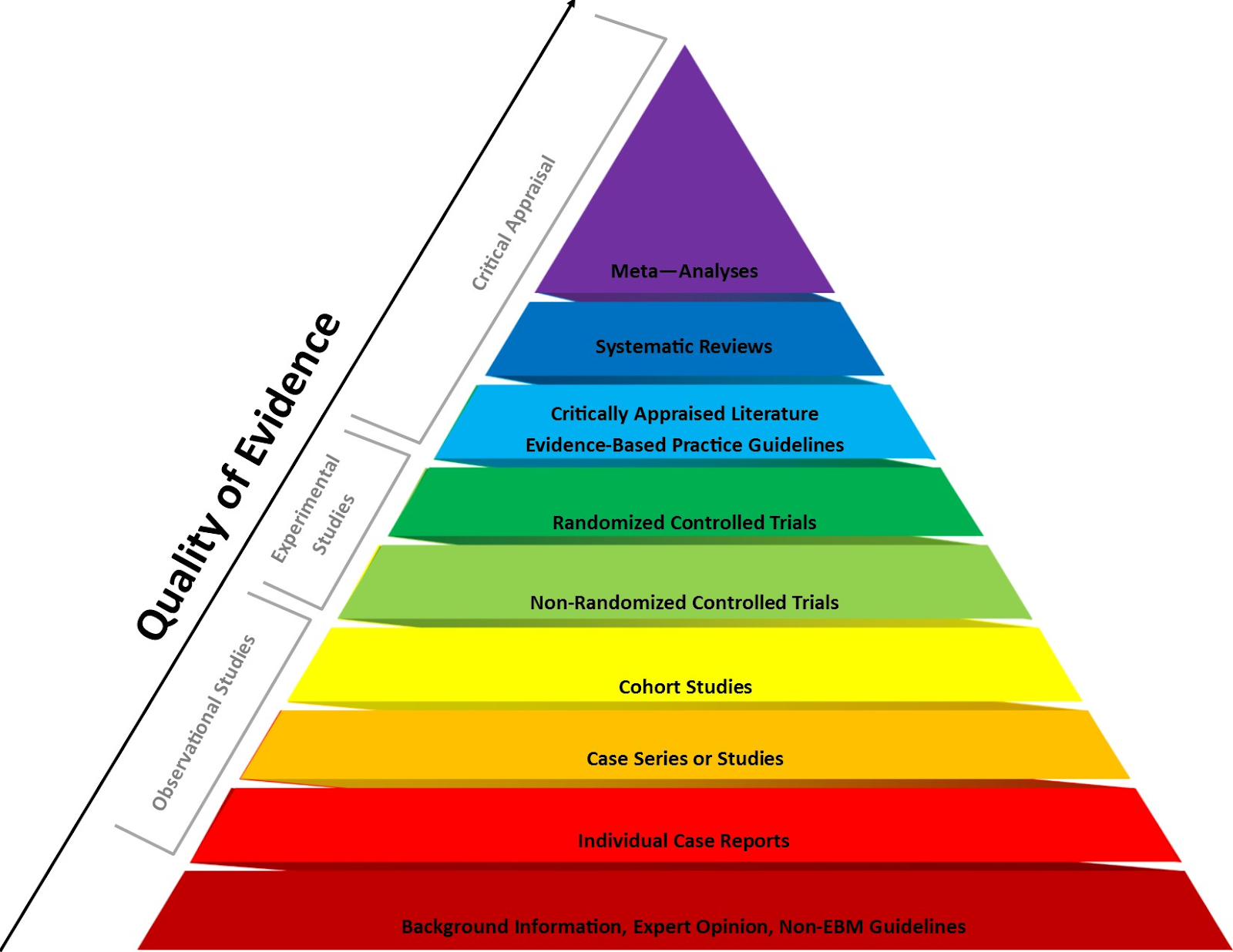
Advocates for mask mandates simply don’t have the highest-levels of scientific evidence to support their arguments. They can only cite low-level science – retrospective observational studies.
Evidence hierarchies are often applied in evidence-based practices and are integral to decision making in medicine and the practice of evidence-based medicine (EBM). The following is from the Wikipedia definition and description of this issue:
A hierarchy of evidence (or levels of evidence) is a heuristic used to rank the relative strength of results obtained from scientific research. There is broad agreement on the relative strength of large-scale, epidemiological studies. More than 80 different hierarchies have been proposed for assessing medical evidence.[1] The design of the study (such as a case report for an individual patient or a blinded randomized controlled trial) and the endpoints measured (such as survival or quality of life) affect the strength of the evidence. In clinical research, the best evidence for treatment efficacy is mainly from meta-analyses of randomized controlled trials (RCTs).[2][3] Typically, systematic reviews of completed, high-quality randomized controlled trials – such as those published by the Cochrane Collaboration – rank as the highest quality of evidence above observational studies, while expert opinion and anecdotal experience are at the bottom level of evidence quality.[2][4]
- Siegfried T (2017-11-13). “Philosophical critique exposes flaws in medical evidence hierarchies”. Science News. Retrieved 2018-05-16.
- Shafee, Thomas; Masukume, Gwinyai; Kipersztok, Lisa; Das, Diptanshu; Häggström, Mikael; Heilman, James (28 August 2017). “Evolution of Wikipedia’s medical content: past, present and future”. Journal of Epidemiology and Community Health. 71 (11): jech–2016–208601. doi:10.1136/jech-2016-208601. ISSN 0143-005X. PMC 5847101. PMID 28847845.
- Straus SE, Richardson WS, Glasziou P, Haynes RB (2005). Evidence-based Medicine: How to Practice and Teach EBM (3rd ed.). Edinburgh: Churchill Livingstone. pp. 102–05. ISBN 978-0443074448.
- Kim Hugel (16 May 2013). “The Journey of Research – Levels of Evidence”. Canadian Association of Pharmacy in Oncology. Retrieved 8 December 2019.
Masks are Ineffective
We are all confused by the mixed messages we have received on mask wearing in the community, businesses, and schools. The issue has become tribal, divisive, and for most, confusing. However, I am not confused. I am fully informed on the scientific research related to masks. After reading this, you will be too. Then, you can make the best decisions for you and your family.
As you will learn from the material that follows, the evidence for and against masks should not be confusing. The evidence is clear, masks are ineffective, unnecessary, and harmful.
What’s happening in the world today, including the misinformation surrounding community mask wearing, is about political agendas, symbolism, and fear, not science.
Mixed Messages from the Experts:
The CoVID-19 pandemic is about viral transmission. Surgical and cloth masks have repeatedly been shown to offer no benefit in the mitigation of transmission and infection caused by viruses like influenza and SARS-CoV-2. Which is exactly why they have never been recommended for use during the seasonal flu outbreak, epidemics, or previous pandemics.
The failure of the scientific literature to support medical masks for influenza and all other viruses, is also why Fauci, the US Surgeon General, the CDC, WHO, and pretty much every infectious disease expert stated that wearing masks won’t prevent transmission of SARS CoV-2. Although the public health “authorities” flipped, flopped, and later changed their recommendations, the science did not change, nor did new science appear that supported the wearing of masks in public. In fact, the most recent systemic analysis once again confirms that masks are ineffective in preventing the transmission of viruses like CoVID-19: https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
If the scientific literature demonstrated that masks were effective, then why, early in the pandemic, did public health experts tell the public not to wear them?
I have heard multiple answers to this question and none of them are reasonable. Here are a couple of the explanations that fail to withstand reasonable scrutiny:
- Early in the pandemic, Fauci, the CDC, the U.S. Surgeon General, and CDC Director Redfield, all said that masks were ineffective and would not protect the wearer or other members of the public from SARS-CoV-2, the virus that causes CoVID-19. lied to the public and congress about masks being because they were trying to protect the supply of masks for health care workers.
- Early in the pandemic, Fauci, et al, actually told the truth about what years of scientific research overwhelmingly concluded: medical masks don’t work to prevent the transmission or infection of viral respiratory pathogens.
- About a month later, for reasons that appear to have more to do with being lobbied by unnamed interest groups, they all began back-pedaling and claiming that what they said previously was actually a lie, but they lied because they were trying to protect the PPE supply for health care workers.
- Absolutely NO NEW research appeared to counter the forty years of meta-analyses and systemic reviews of many randomized controlled trials that concluded that masks don’t work to prevent the transmission of upper respiratory viruses.
- Several low-level evidence, retrospective observational, mechanistic studies, and ridiculous “masked hamster cage” studies appeared in the scientific literature.
- The opinions and theories these studies offered were interesting and worthy of consideration, but they failed to explain or counter the large body of prior high-level evidence. In this paper, I will show that none of these observational studies or mechanistic theories countered the large body of high-level evidence built on years of meta-analyzed and systemically reviewed multiple randomized controlled trials
Redfield, Fauci, Birx, the U.S. Surgeon General, the CDC, and the WHO have been terribly inconsistent, confusing, and flip-flopping on masks throughout the pandemic
We were frequently confused by the mixed messages coming from public health agencies. Early in the pandemic Dr. Fauci, the U.S. Surgeon General, and the WHO all told the public, in no uncertain terms, not to wear masks. Then, over the course of the next several weeks and months, the CDC twice changed their recommendations, as did the WHO, and the two agencies’ recommendations consistently contradicted each other!
CDC: On June 4, 2020, the CDC published guidance indicating that masks do not deter the spread of Covid-19 after as little as fifteen minutes of exposure to someone with symptoms. CDC, Public Health Guidance for Community-Related Exposure, updated July 31, 2020. https://www.cdc.gov/coronavirus/2019-ncov/php/public-health-recommendations.html
WHO: While recommending the wearing of masks for health professionals, the World Health Organization acknowledged that there is no evidence that mask wearing prevents the spread of Covid-19 and that the science simply does not support requiring otherwise healthy people to wear face masks all day.
“At present, there is no direct evidence (from studies on COVID-19 and in healthy people in the community) on the effectiveness of universal masking of healthy people in the community to prevent infection with respiratory viruses, including COVID-19.” World Health Organization (WHO), Advice on the use of masks in the context of COVID-19, Interim Guidance (June 5, 2020) at 6. https://www.who.int/publications/i/item/advice-on-the-use-of-masks-in-the-community-during-home-care-and-in-healthcare-settings-in-the-context-of-the-novel-coronavirus-(2019-ncov)-outbreak
WHO also acknowledged some of the risks long-term mask use poses to health workers and others:
- self-contamination due to the manipulation of the mask by contaminated hands;
- potential self-contamination that can occur if medical masks are not changed when wet, soiled or damaged;
- possible development of facial skin lesions, irritant dermatitis or worsening acne, when used frequently for long hours
- masks may be uncomfortable to wear;
- false sense of security, leading to potentially less adherence to well recognized preventive measures such as physical distancing and hand hygiene;
- risk of droplet transmission and of splashes to the eyes, if mask wearing is not combined with eye protection;
- disadvantages for or difficulty wearing them by specific vulnerable populations such as those with mental health disorders, developmental disabilities, the deaf and hard of hearing community, and children;
- difficulty wearing them in hot and humid environments.
Public Health Authorities changed their minds, but the science did not change. So, what changed their minds?
More than 40 years of science has consistently concluded that masks don’t work. No new science emerged to counter this conclusion. So, what is the basis for the change in direction that emerged from our public health experts?
The following is the Twitter post from Deborah Cohen, UK correspondent for BBC Newsnight and 2019 British Journalism Award winner, indicates that her investigation of the WHO change from not recommending masks to recommending masks had everything to do with politics and lobbying:
Medically qualified, UK Correspondent @BBCNewsnight | 2019 British Journalism Award winner
“We had been told by various sources WHO committee reviewing the evidence had not backed masks but they recommended them due to political lobbying. This point was put to WHO who did not deny. We said some people think we should not wait for RCTs before putting policies in place”
The ineffectiveness of face masks in stemming the spread of viral respiratory diseases, including Covid-19, is widely known and acknowledged in the scientific and medical literature and scientific communities. Therefore, it seems that the transition in public health recommendations to promote widespread mask mandates was based on a combination of low-level observational studies, speculative mechanistic studies, fear, and, most of all, POLITICS, NOT SCIENCE.
To clear up the confusion, I will argue that the scientific evidence not only does not support the community wearing of face masks, but the evidence shows that healthy people wearing face masks pose serious health risks to wearers.
The Evidence AGAINST Masks
Big Data Analysis of 25 U.S. States and 23 Countries Concludes, “Neither Lockdowns nor Mask Mandates Lead to Reduced COVID Transmission Rates or Deaths”
A new National Bureau of Economic Research (NBER) working paper by Andrew Atkeson, Karen Kopecky, and Tao Zha focused on countries and U.S. states with more than 1,000 COVID deaths as of late July. This analysis is the largest and most comprehensive analysis of the largest datasets to date. In all, the study included 25 U.S. states and 23 countries.
The paper’s conclusion is that the data trends indicate that nonpharmaceutical interventions (NPIs) – such as lockdowns, closures, travel restrictions, stay-home orders, event bans, quarantines, curfews, and mask mandates – do not seem to affect virus transmission rates overall.
Systemic Reviews and Meta-Analysis of Multiple Randomized Controlled Trials Concludes that Face Masks Fail to Prevent Transmission of Viral Respiratory Pathogens
One of the largest and highest level of evidence studies on the effectiveness of face masks on the transmission of respiratory viruses, which was recently released by the CDC, is Jingyi Xiao, et al., Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings— Personal Protective and Environmental Measures, Emerging Infectious Diseases, Vol. 26, No. 5, (May 2020). https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
- This CDC meta-analysis found that face masks failed to provide a significant reduction to virus transmission.
- “In our systematic review, we identified 10 [Randomly Controlled Trials] that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks.”
- There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure.
- Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.
Mandates for children to wear face masks fails even a rational basis test, and is clearly not in a child’s best interest, when assessed through a factual, evidence-based analysis, rather than a fear-based lens. It is simply not rational to believe that face masks will be properly and studiously worn by young children for up to ten hours in a school day.
In fact, the overwhelming weight of scientific literature to date establishes that face masks do not prevent the spread of COVID-19 by, to, or from, children.
- Radonovich, L.J. et al., N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial, JAMA. 2019; 322(9): 824–833. doi:10.1001/jama.2019.11645, 2019. https://jamanetwork.com/journals/jama/fullarticle/2749214
- “Among 2862 randomized participants, 2371 completed the study and accounted for 5180 HCW-seasons. … Among outpatient health care personnel, N95 respirators vs medical masks as worn by participants in this trial resulted in no significant difference in the incidence of laboratory-confirmed influenza.”;
- Long, Y. et al., Effectiveness of N95 respirators versus surgical masks against influenza: A systematic review and meta‐analysis, J Evid Based Med. 2020; 1‐ 9. https://doi.org/10.1111/jebm.12381
- A total of six [Randomized Controlled Trials] involving 9171 participants were included.
- There were no statistically significant differences in preventing laboratory‐confirmed influenza, laboratory‐confirmed respiratory viral infections, laboratory‐confirmed respiratory infection and influenza-like illness using N95 respirators and surgical masks.
- Meta‐analysis indicated a protective effect of N95 respirators against laboratory‐confirmed bacterial colonization.
- The use of N95 respirators compared with surgical masks is not associated with a lower risk of laboratory‐confirmed influenza.
- See e.g., Patrick Saunders-Hastings, et, al., Effectiveness of personal protective measures in reducing pandemic influenza transmission: A systematic review and meta-analysis, Epidemics, v. 20 (September 2017)
- This systemic review found “face mask use provided a non significant protective effect . . . against 2009 pandemic influenza infection.” https://www.sciencedirect.com/science/article/pii/S1755436516300858
- An April 2020 review by the Norwich School of Medicine found that “the evidence is not sufficiently strong to support widespread use of face masks”, but supports the use of masks by “particularly vulnerable individuals when in transient higher risk situations.”
- Brainard, et al., face masks and similar barriers to prevent respiratory illness such as COVID-19: A rapid systematic review, April 6, 2020. https://www.medrxiv.org/content/10.1101/2020.04.01.20049528v1
- Dr. Russell Blaylock, a nationally recognized board-certified neurosurgeon, health practitioner, author, and lecturer warns that not only do face masks fail to protect the healthy from getting sick, but they also create serious health risks to the wearer.
- Dr. Russell Blaylock, Blaylock: Face Masks Pose Serious Risks To The Healthy, Technocracy News & Trends, (posted May 11, 2020). https://www.technocracy.news/blaylock-face-masks-pose-serious-risks-to-the-healthy/
- [Recent studies] found that about a third of the [healthcare] workers developed headaches with use of the mask, most had preexisting headaches that were worsened by the mask wearing, and 60% required pain medications for relief. As to the cause of the headaches, while straps and pressure from the mask could be causative, the bulk of the evidence points toward hypoxia and/or hypercapnia as the cause. That is, a reduction in blood oxygenation (hypoxia) or an elevation in blood C02 (hypercapnia).
- It is known that the N95 mask, if worn for hours, can reduce blood oxygenation as much as 20%, which can lead to a loss of consciousness.
- The importance of these findings is that a drop in oxygen levels (hypoxia) is associated with an impairment in immunity. Studies have shown that hypoxia can inhibit the type of main immune cells used to fight viral infections called the CD4+ T-lymphocyte.
- This occurs because the hypoxia increases the level of a compound called hypoxia inducible factor-1 (HIF-1), which inhibits T-lymphocytes and stimulates a powerful immune inhibitor cell called the Tregs.
- This sets the stage for contracting any infection, including COVID-19 and making the consequences of that infection much graver. In essence, your mask may very well put you at an increased risk of infections and if so, having a much worse outcome. Id.
- See also Denis G. Rancourt, PhD, Masks Don’t Work: A review of science relevant to COVID-19 social policy, Ontario Civil Liberties Association, April 11, 2020. https://www.researchgate.net/publication/340570735
- There have been extensive randomized controlled trial (RCT) studies, and meta-analysis reviews of RCT studies, which all show that masks and respirators do not work to prevent respiratory influenza-like illnesses, or respiratory illnesses believed to be transmitted by droplets and aerosol particles.
- Furthermore, the relevant known physics and biology, which I review, are such that masks and respirators should not work. It would be a paradox if masks and respirators worked, given what we know about viral respiratory diseases: The main transmission path is long residence-time aerosol particles (< 2.5 µm), which are too fine to be blocked, and the minimum-infective-dose is smaller than one aerosol particle.
- Jacobs, J. L. et al. (2009) Use of surgical face masks to reduce the incidence of the common cold among health care workers in Japan: A randomized controlled trial, American Journal of Infection Control, Volume 37, Issue 5, 417 – 419 https://www.ncbi.nlm.nih.gov/pubmed/19216002
- “N95-masked health-care workers (HCW) were significantly more likely to experience headaches.”
- “Face mask use in HCW was not demonstrated to provide benefit in terms of cold symptoms or getting colds.”
- Cowling, B. et al., Face masks to prevent transmission of influenza virus: A systematic review, Epidemiology and Infection, 138(4), 449-456. doi:10.1017/S0950268809991658 2010. https://www.cambridge.org/core/journals/epidemiology-and-infection/article/face-masks-to prevent-transmission-of-influenza-virus-a-systematic
- “None of the studies reviewed showed a benefit from wearing a mask, in either [Health Care Workers] or community members in households . . . .”
- bin-Reza et al., The use of masks and respirators to prevent transmission of influenza: a systematic review of the scientific evidence, Influenza and Other Respiratory Viruses 6(4), 257–267, 2012. https://onlinelibrary.wiley.com/doi/pdf/10.1111/j.1750-2659.2011.00307.x
- “There were 17 eligible studies. … None of the studies established a conclusive relationship between mask ⁄ respirator use and protection against influenza infection.”
- Offeddu, V. et al., Effectiveness of Masks and Respirators Against Respiratory Infections in Healthcare Workers: A Systematic Review and Meta-Analysis, Clinical Infectious Diseases, Volume 65, Issue 11, 1 December 2017, Pages 1934–1942. https://doi.org/10.1093/cid/cix681
- “Self-reported assessment of clinical outcomes was prone to bias. Evidence of a protective effect of masks or respirators against verified respiratory infection (VRI) was not statistically significant”
In fact, many physicians and researchers now believe that, because the ineffectiveness of face masks in stemming the spread of Covid-19 is so widely known and acknowledged in the scientific and medical communities, the goal of widespread mask mandates is based entirely on low-level observational studies, speculative mechanistic studies, fear, and politics, not science.
- See Michael Klompas, M.D., M.P.H., et. al., Universal Masking in Hospitals in the Covid-19 Era, New England Journal of Medicine, N Engl J Med 2020; 382:e63 (May 21, 2020). https://www.nejm.org/doi/full/10.1056/NEJMp2006372
- We know that wearing a mask outside health care facilities offers little, if any, protection from infection. . . It is also clear that masks serve symbolic roles. Masks are not only tools, they are also talismans that may help increase health care workers’ perceived sense of safety, well being, and trust in their hospitals. Although such reactions may not be strictly logical, we are all subject to fear and anxiety, especially during times of crisis. One might argue that fear and anxiety are better countered with data and education than with a marginally beneficial mask.
- See also Lisa M Brosseau, ScD, Margaret Sietsema, PhD, COMMENTARY: Masks-for-all for COVID-19 not based on sound data, Center for Infectious Disease Research and Policy, University of Minnesota, April 1, 2020. https://www.cidrap.umn.edu/news-perspective/2020/04/commentary-masks-all-covid-19-not based-sound-data
- Dr. Brosseau is a national expert on respiratory protection and infectious diseases and professor (retired), University of Illinois at Chicago. Dr. Sietsema is also an expert on respiratory protection and an assistant professor at the University of Illinois at Chicago. They made the following key points in their commentary:
“We do not recommend requiring the general public who do not have symptoms of COVID-19-like illness to routinely wear cloth or surgical masks because:
- There is no scientific evidence they are effective in reducing the risk of SARS-CoV-2 transmission.
- Their use may result in those wearing the masks to relax other distancing efforts because they have a sense of protection.
- We need to preserve the supply of surgical masks for at-risk healthcare workers.
Sweeping mask recommendations—as many have proposed—will not reduce SARS-CoV-2 transmission, as evidenced by the widespread practice of wearing such masks in Hubei province, China, before and during its mass COVID-19 transmission experience earlier this year.
Our review of relevant studies indicates that cloth masks will be ineffective at preventing SARS-CoV-2 transmission, whether worn as source control or as PPE.
Masks as means of “Source Control” – No, My Mask Does Not Protect You From Me
The public is being repeatedly misinformed by catchy (guilt and fear based) marketing messages designed to promote the social responsibility (or guilt) to wear masks as a form of source control: “I wear my mask for you and you wear your mask for me.”
Where is the evidence for these claims? On the websites where these unscientific marketing messages are found, there are never references to science that supports the claims. In fact, despite almost everything that has been drilled into the public psyche regarding masks, has little to know basis in science and absolutely no robust support from the highest-level evidence based research. Masks have never been proven to protect either the wearer or the community from the transmission of respiratory pathogens. Mask mandates during a pandemic are opposed by decades of high level science.
Simply put, the public is being misled by fraudulent claims supported with weak pseudoscience.
The fallacious argument: “Well, if masks don’t work, then why do surgeons wear them?”
I’m an ophthalmic surgeon. I specialize in ocular immunology, inflammation, and infectious disease. I’ve performed over 10,000 surgical procedures wearing a surgical mask. I have suffered the detrimental effects that masks caused to my mental and physical function during long surgeries. Because most of the surgeries I performed were microscopic procedures that required fine motor skills, I changed my mask frequently to prevent the detrimental effects of arterial deoxygenation.
However, these facts alone don’t qualify me as an expert on the matter. What qualifies me is my experience as an editor of a medical journal, the fact that I’ve peer-reviewed thousands of pre-print research articles, that I am an expert at reading medical research, distinguishing good science from bad, and separating fact from fiction.
Believe me, the medical literature is filled with bad fiction masquerading as medical science. It is very easy to be deceived by bad science.
Since the beginning of the pandemic I’ve read hundreds of studies on the science of medical masks. Based on extensive review and analysis, there is no question in my mind that healthy people should not be wearing surgical or cloth masks. Nor should we be recommending universal masking of all members of the population. That recommendation is not supported by the highest level of scientific evidence.
First, the premise that surgeons wearing masks serves as evidence that “masks must work to prevent viral transmission” is a logical fallacy. I would classify this claim as an argument of false equivalence, or comparing “apples to oranges.” Surgical masks offer no benefit in protecting patients from the surgeon’s respiratory droplets contaminating the surgical field and the exposed tissues of surgical patients.
Surgeons well-versed in the scientific research regarding medical masks, especially the systemic reviews published by the Cochrane Collaboration Wound Group, know that surgical face masks provide no benefit in the prevention of surgical wound infections.[R][R] Surgeons with experience wearing surgical masks during long surgeries have undoubtedly experienced and understand the detrimental effects masks have on respiration, blood oxygenation, mental, and physical performance. For these science-based reasons, there is a worldwide trend towards surgeons and operating room staff no longer wearing surgical masks during “clean surgery” cases.
Nevertheless, many surgeons continue to wear face masks during clean surgery cases and outpatient minor procedures. We do so more for symbolic purposes, habit, tradition, or, not infrequently, because of institutional ignorance. That is, we are forced to wear masks because it is the ignorant, anti-science policy of the hospital or surgery center where we perform our surgeries.
Although wearing a mask during a clean surgery is unnecessary, there are other surgical cases in which surgical masks, eye protection, and face shields are still a good idea. For example, cases in which bone saws, drills, and other surgical power tools can expose the surgical team to splashes and splatters from the patient’s bodily fluids.
If a surgeon were sick, especially with a viral infection, they would not perform surgery as they know the virus would NOT be stopped by their surgical mask.
Another area of “false equivalence” has to do with the environment in which the masks are worn. The environments in which surgeons wear masks minimize the adverse effects surgical masks have on their wearers.
Unlike the public wearing masks in the community, surgeons work in sterile surgical suites equipped with heavy duty air exchange systems that maintain positive pressures, exchange and filter the room air at a very high level, and increase the oxygen content of the room air. These conditions limit the negative effects of masks on the surgeon and operating room staff. And yet despite these extreme climate control conditions, clinical studies demonstrate the negative effects (lowering arterial oxygen and carbon dioxide rebreathing) of surgical masks on surgeon physiology and performance.
Surgeons and operating room personnel are well trained, experienced, and meticulous about maintaining sterility. We only wear fresh sterile masks. We don the mask in a sterile fashion. We wear the mask for short periods of time and change it out at the first signs of the excessive moisture build up that we know degrades mask effectiveness and increases their negative effects. Surgeons NEVER reuse surgical masks, nor do we ever wear cloth masks.
The public is being told to wear masks for which they have not been trained in the proper techniques. As a result, they are mishandling, frequently touching, and constantly reusing masks in a way that increases contamination and are more likely than not to increase transmission of disease.
Just go watch people at the grocery story or Walmart and tell me what you think about the effectiveness of masks in the community.
If you can’t help but believe and trust the weak retrospective observational studies and confused public health “authorities” lying to you about the benefits and completely ignoring the risks of medical masks, then you should at least reject the illogical anti-science recommendation to block only 2 of the 3 ports of entry for viral diseases. Masks only cover the mouth and nose. They do not protect the eyes.
Surgeons and Surgical Masks: Little to No Benefit of Surgical Masks During Surgery
While it may go against “conventional wisdom,” and may seem counterintuitive to those who are not involved in scientific research, the actual scientific evidence does not support the proposition that wearing a mask is an effective method of source control to prevent the spread of infection.
Many surgeons are surprised to learn that when surgical masks are put to the test in randomized controlled trials, they fail to demonstrate benefit. In fact, surgical masks have repeatedly failed to provide evidence of effectiveness as a means of “source control,” even in the one environment where they are so steadfastly adhered to: the operating room. Simply put, based on the actual science face masks have repeatedly been found to be ineffective as a means of source control. Face masks do not protect against the very risk for which the Defendants are forcing small children to wear face masks all day: source control.
- In 2014, the Cochrane Collaboration “Wounds Group” reviewed all research related to the topic of effectiveness of face masks for preventing surgical wound infections.
- Lipp, A. and Edwards, P., Disposable surgical face masks for preventing surgical wound infection in clean surgery (Review), Cochrane Database of Systematic Reviews 2014, Issue 2. Art. No.: CD002929. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD002929.pub2/epdf/full
- “Three [randomized controlled] trials were included, involving a total of 2113 [surgical team] participants. There was no statistically significant difference in infection rates between the masked and unmasked group in any of the trials.”
- In 2016, the Cochrane Collaboration “Wounds Group” revisited the topic of effectiveness of face masks for preventing surgical wound infections again in 2016. In this updated review they added any new studies on the topic that entered the literature since their 2014 review (above).
- Vincent, M. & Edwards, P., Disposable surgical face masks for preventing surgical wound infection in clean surgery, Cochrane Database of Systematic Reviews 2016, Issue 4, Art. No.: CD002929. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD002929.pub3/epdf/full
- “Overall, we found very few studies and identified no new trials for this latest update. We analysed a total of 2106 participants from the three studies we found.”
- “All three [randomized controlled trials] showed that wearing a face mask during surgery neither increases nor decreases the number of wound infections occurring after surgery. We conclude that there is no clear evidence that wearing disposable face masks affects the likelihood of wound infections developing after surgery.”
- See, e.g., Neil W. M. Orr, M.D., Mchir, FRCS, Is a mask necessary in the operating theatre?, Annals of the Royal College of Surgeons of England, vol. 63, 1981. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2493952/pdf/annrcse01509-0009.pdf
- This six month long study showed a significant decrease in the rate of patient infections when masks were NOT worn in an operating theater.
- Ritter, MA, et al., The operating room environment as affected by people and the surgical face mask. Clinical Orthopaedics and Related Research: September 1975 – Volume 111 – Issue – p 147-150. https://journals.lww.com/clinorthop/Citation/1975/09000/The_Operating_Room_Environment\_as _ Affected_by.20.aspx
- “The wearing of a surgical face mask had no effect upon the overall operating room environmental contamination…”
- Da Zhou et al., Unmasking the surgeons: the evidence base behind the use of face masks in surgery, Journal of the Royal Society of Medicine; 2015, Vol. 108(6) 223–228. https://journals.sagepub.com/doi/pdf/10.1177/0141076815583167
- The paper analyzed numerous studies.
- The use of surgical face masks is ubiquitous in surgical practice. Face Masks have long been thought to confer protection to the patient from wound infection and contamination from the operating surgeon and other members of the surgical staff… However, overall there is a lack of substantial evidence to support claims that face masks protect either patient or surgeon from infectious contamination. (emphasis added)
- Zahid Mehmood Bahli, Does evidence based medicine support the effectiveness of surgical face masks in preventing postoperative wound infections in elective surgery?, J Ayub Med Coll Abbottabad 2009; 21(2). http://www.ayubmed.edu.pk/JAMC/PAST/21-2/Zahid.pdf
-
- “No significant difference in the incidence of postoperative wound infection was observed between masks group and groups operated with no masks. There was no increase in infection rate in 1980 when masks were discarded. In fact there was a significant decrease in infection rate.” (emphasis added)
- Ana E. Figueiredo, et. al., Bag Exchange in Continuous Ambulatory Peritoneal Dialysis Without Use of a Face Mask: Experience of Five Years, Renal Unit, Hospital São Lucas, Porto Alegre, Brazil. http://www.advancesinpd.com/adv01/21Figueiredo.htm
- “Peritonitis rates reported during our observation period are compatible with those seen in other centers and support the hypothesis that routine use of a face mask during CAPD bag exchange may be unnecessary.”
- M.W. Skinner, B.A Sutton, Do Anaesthetists Need to Wear Surgical Masks in the Operating Theatre? A Literature Review with Evidence-Based Recommendations, Anaesthesia and Intensive Care, Vol. 29, No. 4, August 2001. https://journals.sagepub.com/doi/pdf/10.1177/0310057X0102900402
- The evidence for discontinuing the use of surgical face masks would appear to be stronger than the evidence available to support their continued use. . . .
- There is little evidence to suggest that the wearing of surgical face masks by staff in the operating theatre decreases postoperative wound infections.
- Published evidence indicates that postoperative wound infection rates are not significantly different in unmasked versus masked theatre staff.
- However, there is evidence indicating a significant reduction in postoperative wound infection rates when theatre staff are unmasked.
- Currently there is no evidence that removing masks presents any additional hazard to the patient. (emphasis added).
- See Eva Sellden, M.D., Ph.D., Is Routine Use of a Face Mask Necessary in the Operating Room?, Anesthesiology 2010; 113:1447, the American Society of Anesthesiologists, Inc. https://pubs.asahq.org/anesthesiology/article/113/6/1447/9572/Is-Routine-Use-of-a-Face-Mask Necessary-in-the
- “Our decision to no longer require routine surgical masks for personnel not scrubbed for surgery is a departure from common practice. But the evidence to support this practice does not exist . . . .”
Cloth Masks are Ineffective and May Increase the Risk of Transmission
Cloth masks are absolutely ineffective. Worst yet, they may increase the incidence of disease in wearers and the population.
Despite the high-level scientific evidence against cloth masks, the CDC made the inexcusable mistake of telling us cloth masks worked. They even provided directions on their website for making homemade cloth masks.
A July 2020 review by the University of Oxford, Centre for Evidence-Based Medicine found that there is no evidence that cloth masks are at all effective against virus infection or transmission.
- Jefferson, Tom & Heneghan, Carl, Masking lack of evidence with politics, Centre for Evidence-Based Medicine, July 23, 2020. https://www.cebm.net/covid-19/masking-lack-of-evidence-with-politics/
A July 2020 study by Japanese researchers found that cloth masks “offer zero protection against coronavirus.”
- Naoya Kon, Cloth face masks offer zero shield against virus, a study shows, The Asahi Shimbun, study by Kazunari Onishi. http://www.asahi.com/ajw/articles/13523664
- “This experiment reconfirmed that wearing cloth and gauze masks can’t prevent virus infection.”
In an August 2020 article, Denis G. Rancourt, PhD, a Researcher, Ontario Civil Liberties Association, debunks supposed “studies” purporting to support compelled face mask use for the general population.
- See Rancourt, Face masks, lies, damn lies, and public health officials: “A growing body of evidence” August 2020. https://www.researchgate.net/publication/343399832_Face_masks_lies_damn_lies_and_public_hea lthofficialsAgrowingbodyofevidence
- “[T]here is no policy-grade evidence to support forced masking on the general population, . . . all the latest-decade’s policy-grade evidence points to the opposite: NOT recommending forced masking of the general population.”);
- No [randomized controlled trial] study with verified outcome shows a benefit for [health-care workers] or community members in households to wearing a mask or respirator. There is no such study. There are no exceptions. Likewise, no study exists that shows a benefit from a broad policy to wear masks in public (more on this below).
- Furthermore, if there were any benefit to wearing a mask, because of the blocking power against droplets and aerosol particles, then there should be more benefit from wearing a respirator (N95) compared to a surgical mask, yet several large meta-analyses, and all the RCT, prove that there is no such relative benefit.
- Masks and respirators do not work. (emphasis added);
- Denis G. Rancourt, PhD, Masks Don’t Work: A Review of Science Relevant to COVID-19 Social Policy, River Cities Reader, June 11, 2020. https://www.rcreader.com/commentary/masks-dont-work-covid-a-review-of-science-relevant-to covide-19-social-policy
- see also, Todd McGreevy, Still No Conclusive Evidence Justifying Mandatory Masks, River Cities Reader, August 12, 2020. https://www.rcreader.com/commentary/still-no-conclusive-evidence-justifying-mandatory-masks
I presented a partial list of the various meta-analyses and systemic reviews of multiple randomized controlled trials (RCTs). The studies represent the highest level of evidence that masks don’t work.
This WHO commissioned study is the best counter to my arguments. To any trained researcher, this study falls far short of countering decades of the science previously presented.
Advocates for mask mandates simply don’t have the highest-levels of scientific evidence to support their arguments. They can only cite low-level science – retrospective observational studies. The WHO study is a cleverly disguised example of low-level garbage dressed up to appear better than what it is. You have to examine the details to detect the weak deception.
The Evidence FOR Masks
The best evidence for masks was commissioned by the WHO and published in the Lancet in June 2020. The title, “Physical Distancing, Face Masks, and Eye Protection to Prevent Person-to-Person Transmission of SARS-CoV-2 and COVID-19: A Systematic Review and Meta-Analysis,” sounds like high-level scientific evidence. After all, systemic reviews and meta-analyses are typically considered the epitome of evidence based medicine. However, don’t be deceived by the authors’ deceptive attempts to elevate the relevancy of this study. This systemic review/meta-analysis was entirely comprised of low-level observational studies. No high-level randomized controlled trials were included.
No matter how much the authors attempt to deceive or embellish the study’s relevance with its “dressed up” title, the fact remains, this study still amounts to nothing more than a steaming pile of weak evidence. No matter how much the authors and the WHO want this study to represent high-level evidence for masking world populations, it simply cannot be considered to be more than the sum of its low level parts.
Furthermore, the study is seriously flawed with serious misrepresentations and misinterpretations of the data. The flaws, errors, and mistakes in this analysis of 29 observational studies should lead to its retraction from the Lancet. The flaws are buried in the data tables, therefore, it is missed by those that do little more than read titles and conclusions. Which is exactly why studies like this should be subjected to thorough and independent peer-review before publication.
Scientists all over the world are raising concerns and speaking against the study and demanding its retraction. For example, University of Toronto epidemiology professor Peter Jueni called the WHO study “methodologically flawed” and “essentially useless”.
Garbage-in-garbage out: the June 2020 WHO commissioned study of masks published in The Lancet.
- Source: Chu, Derek K., Elie A. Akl, Stephanie Duda, Karla Solo, Sally Yaacoub, Holger J. Schünemann, and COVID-19 Systematic Urgent Review Group Effort (SURGE) study authors. 2020. “Physical Distancing, Face Masks, and Eye Protection to Prevent Person-to-Person Transmission of SARS-CoV-2 and COVID-19: A Systematic Review and Meta-Analysis.” The Lancet 395 (10242): 1973–87.
Summary: the WHO-commissioned meta-study on the effectiveness of facemasks and social distancing, published in The Lancet, is seriously flawed and should be retracted.
This study is nothing more than a seriously flawed meta-analysis of 29 weak observational studies. None of the trials were randomized controlled trials. No matter how thoroughly you sift through the weak, low-level of evidence, observational studies, in the end, all you end up with is weak, easily biased, and essentially unusable evidence.
For a more comprehensive analysis of the flaws and a thorough debunking of the relevance of this study, read this: WHO Mask Study Seriously Flawed, Swiss Policy Research (Sept. 9, 2020), copied here:
Update: A US analyst has reviewed all 29 studies and found numerous additional mistakes.
A. General flaws
- Of the 29 studies analyzed by the Lancet meta-study, seven studies are unpublished and non-peer-reviewed observational studies. Non-peer reviewed studies should not be used to guide clinical practice according to the medRxiv disclaimer. [3] [4] [31] [36] [37] [40] [70]
- Of the 29 studies considered by the meta-study, only four are about the SARS-CoV-2 virus; the other 25 studies are about the SARS-1 virus or the MERS virus, both of which have very different transmission characteristics: they were transmitted almost exclusively by severely ill hospitalized patients and not by community transmission.
- Of the four studies relating to the SARS-CoV-2 virus, two were misinterpreted by the Lancet meta-study authors[44] [70], one is inconclusive [37], and one is about N95 (FFP2) respirators and not about medical masks or cloth masks (see detailed analysis below).
- Despite the weakness, misinterpretations, and inapplicability, the Lancet meta-study is used to guide global facemask policy for the general population. However, of the 29 studies considered by the meta-study, only three are classified as relating to a non-health-care (i.e. community) setting. Of these three studies, one is misclassified [50] (relating to masks in a hospital environment), one showed no benefit of facemasks [69], and one is a poorly designed retrospective study about SARS-1 in Beijing based on telephone interviews [74]. None of these studies pertained to SARS-CoV-2.
- The authors of the Lancet meta-study acknowledge that the certainty of the evidence regarding facemasks is “low” as all of the studies are observational and none is a randomized controlled trial (RCT).
- The WHO itself admitted that its updated facemask policy guidelines were based not on new evidence but on “political lobbying”.
B. Study misinterpretations
As mentioned above, several studies have been misinterpreted by the authors of the meta-study. All of the misinterpretations resulted in falsely claiming or exaggerating a benefit of facemasks. In the following, only the four studies relating to SARS-CoV-2 are reviewed. (HCW: health care worker)
- Heinzerling et al. [44]: The meta-study claims that 0 of 31 HCW wearing a facemask and 3 of 6 HCW not wearing a facemask got infected. This is not correct.The study showed that 0 of 3 HCW wearing a facemask and 3 of 34 HCW not wearing a facemask got infected. This result was not statistically significant (p=0.73). Moreover, of the 3 HCW who got infected, one reported wearing a facemask “most of the time”, but the meta-study classified this HCW as “not wearing a facemask”.
- Wang et al. [41]: This study, which did show a benefit of facemasks, was about N95 (FFP2) respirators in a health-care setting, not about medical masks or cloth masks.
- Wang et al. [70]: The meta-study claims that 1 of 1286 HCW wearing a facemask and 119 of 4036 wearing “no facemask” got infected. This is not correct.According to the study, 78.3% (94/120) of infected HCWs were in fact wearing a surgical mask, and only 20.8% (25/120) did not wear any mask when exposed to the source of infection. The “1 of 1286 HCW” mentioned in the meta-study refers to HCW wearing an N95 (FFP2) respirator, not a medical or cloth mask.
- Burke et al. [37]: This study had no results relating to the use of facemasks.
Non-Covid studies were also misinterpreted or misrepresented by the Lancet meta-study authors. For instance, in the case of the non-Covid study with the allegedly biggest impact of masks (Kim et al. [49] about N95 respirators in a hospital with MERS patients), the meta-study authors incorrectly mixed serological and PCR results, again exaggerating the benefit of (N95) masks. The actual results of the Kim et al. study were not statistically significant (p=0.159).
C. Studies relating to “social distancing”
In an additional section, the WHO meta-study evaluated studies on the benefit of “social distancing” measures. However, several independent experts have shown that this section is seriously flawed. The authors again misinterpreted several studies and made several statistical errors.
As with the studies on facemasks, all of these mistakes resulted in falsely claiming or exaggerating a benefit of “social distancing” measures.
For more information on this section, see PubPeer (and links therein) and the CEBM review.
Conclusion
As shown in this analysis, the WHO-commissioned meta-study on the effectiveness of facemasks and social distancing, published in The Lancet, is seriously flawed and should be retracted. Health authorities may want to reconsider their Covid-19 policy guidelines.
Community Use Of Face Masks And COVID-19: Evidence From A Natural Experiment Of State Mandates In The US
https://www.healthaffairs.org/doi/10.1377/hlthaff.2020.00818
Limitations of the Studies Typically Used to Support Masks
- They are all low-level evidence, retrospective observational studies. At the time of my analysis and writing of this paper, none of the studies purporting to support community wearing of masks used high-level randomized clinical trial methodology.
- Cannot distinguish correlation from causation.
- Does not measure face cover use in the community or any measure of compliance.
- Estimates represent the intent-to-treat effects of these mandates, not the individual-level effect of wearing a face mask in public on one’s own COVID-19 risk.
- Did not measure types of masks worn.
- Did not assess adverse effects of masks.
- Did not control for other community-wide and hospital-specific interventions that may have contributed to or confounded their observations, including:
- Declarations of emergency (March 10),
- New hospital policies to restrict visitors (March 12) and elective procedures (March 14),
- School closures
- Hospital restrictions on business travel and on-site working (March 16),
- Local public transportation reductions (March 17),
- Issuance of statewide stay-at-home orders (March 24), and
- Automation of screening and testing (March 30).
Masks are Unnecessary
Fear and Politics are Subverting Science and Reason
Public health officials and the media have been warning us that coronavirus kills not just old or immunocompromised people but young people too. While this is true, it remains extremely rare.
A Pandemic of Fraud and Fear is More Dangerous than the COVID-19 Pandemic
Death rate data from the CDC: COVID-19 Pandemic Planning Scenarios
Table 1. Parameter Values that vary among the five COVID-19 Pandemic Planning Scenarios.

Parameters:
- Scenario 5: Current Best Estimate, R0 = 2.5, 40% asymptomatic
- For a definition of R0, see HealthKnowlege-UK (2020): R0 is “the average number of secondary infections produced by a typical case of an infection in a population where everyone is susceptible.” The average R0 for influenza is said to be 1.28 (1.19–1.37); see the comprehensive review by Biggerstaff et al. (2014).
- According to the CDC’s latest best estimate, 40% of COVID-19 infections are asymptomatic.
- Parameter values are based on data received by CDC through August 8, 2020.
- These estimates are based on age-specific estimates of infection fatality ratios from Hauser, A., Counotte, M.J., Margossian, C.C., Konstantinoudis, G., Low, N., Althaus, C.L. and Riou, J., 2020
Masking Children in Schools is Unnecessary – So Says The Science
School and daycare transmission studies show that transmission of Covid-19 among unmasked children is remarkably low.
German study finds low Covid-19 infection rate in schools. Tests of pupils and teachers in Saxony suggest children may act as brake on infection.
The study by the University hospital in Dresden analysed blood samples from almost 1,500 children and 500 teachers from 13 schools in Saxony, Germany suggests schools may not play as big a role in spreading the virus as some had feared.
“Of the almost 2,000 samples, only 12 had antibodies,” said Reinhard Berner, a professor of paediatrics at the hospital. In other words, in Saxony’s open and unmasked schools 0.6% of school children demonstrated SARS-CoV-2 antibodies.
All cases were asymptomatic. There were no fatalities.
“Children may even act as a brake on infection,” Berner told a news conference, saying “infections in schools had not led to an outbreak, while the spread of the virus within households was also less dynamic than previously thought.”
“For other states with low infection rates, the study suggests schools could be reopened without fear of causing widespread outbreaks of the virus,” Berner said.
Sweden and Finland: 0.05% of children infected by Covid-19
Sweden kept schools open and unmasked during the pandemic, yet their decision to adhere to the science and do what has always been done before, did not lead to a higher rate of infection among their children compared to neighboring Finland, where schools were closed temporarily.
Based on Covid-19 case data collected from each country during the time period, Feb. 24 to June 14, the percentage of children between the ages of 1-19 infected by Covid-19 was the same:
- Sweden: 1,124 cases 0.05%
- Finland: 584 cases 0.05%
Separate studies by Sweden’s Karolinska Institutet (KI), an independent medical research institute, and the European Network of Ombudspersons for Children and Unicef, showed that Swedish children fared better than children in other countries during the pandemic, both in terms of education and mental health.
COVID-19 transmission rate 0.3% among children in schools and nurseries in New South Wales, Australia
The Lancet Child & Adolescent Health: Effective testing and contact tracing is essential for schools to safely open during COVID-19 pandemic, two studies show. The Lancet; August 3, 2020. https://www.eurekalert.org/pub_releases/2020-08/tl-pss080320.php
Real world data from schools where masks were not required or worn demonstrates a remarkably low rate of transmission of SARS-CoV-2. Analysis of COVID-19 case data from 3103 schools and approximately 4600 nurseries in New South Wales demonstrate that schools and nurseries do not pose a high risk for COVID-19 transmission.
Subset analysis found that only 27 children or teachers went to school while they were infectious, with an additional 18 people later becoming infected. Out of 1448 contacts in total, the rate of secondary transmission was found to be 1.2%.
A subset analysis of 7 schools and nurseries that underwent additional investigations including antibody testing, symptom surveys, and extra RT-PCR testing for the virus showed that the transmission rates among children and staff were extremely low:
- child-to-child rate was 0.3%,
- child-to-staff rate was 1.0%
- staff-to-child rate was 1.5%
- staff-to-staff rate was 4.4%.
The researchers noted that this finding suggests that children are less likely to transmit the virus than adults.
While coronavirus is obviously concerning and a very real threat to some people (namely, the elderly and immunocompromised), these data also show that the risk for the rest of the population is extraordinarily low.
Masks are Harmful: 17 Ways That Masks Can Cause Harm
As a physician and former medical journal editor, I’ve carefully read the scientific literature regarding the use of face masks to mitigate viral transmission. I believe the public health experts have community wearing of masks all wrong. Here are a few of the mechanisms by which medical masks can be harmful to their wearers and community wearing of face masks is a very bad idea:
Wearing masks for extended periods increased incidences of headaches and negatively affected work performance.
See Jonathan J.Y. Ong, et al., Headaches Associated With Personal Protective Equipment – A Cross‐Sectional Study Among Frontline Healthcare Workers During COVID‐19, Headache, the Journal of Head and Face Pain (May 2020). https://headachejournal.onlinelibrary.wiley.com/doi/full/10.1111/head.13811
1. Medical masks adversely affect respiratory physiology and function.
-
Masks inhibit air flow into and out of the lungs.
- For people with asthma, chronic obstructive pulmonary disease (COPD), and many other chronic lung diseases, face masks are intolerable to wear as they worsen breathlessness.[R]
- Medical masks lower blood oxygen and raise carbon dioxide such that respiratory rate and depth of breaths are increased.[R]
- Decreasing oxygen and increasing carbon dioxide in the bloodstream stimulates a compensatory response in the respiratory centers of the brain. These changes in blood gases result in increases in both frequency and depth of breaths.
- As masks Increase both the frequency and depth of respirations (breaths), they increase the likelihood that each respiration will contain a larger amount of infectious viral particles. This may worsen the community transmission of CoVID-19 as infected people wearing masks exhale respiratory plumes loaded with greater levels of infectious viral particles. These infectious plumes readily move around the sides, bottom, and top of masks.
- This may also increase the severity of CoVID-19 as the increased tidal volume delivers the viral particles deeper into the lungs.
- These effects are amplified if face masks are contaminated with the viruses, bacteria, or fungi that find their way or opportunistically grow in the warm, moist environment that medical masks quickly become.
2. Medical masks lower oxygen levels in the blood.[R]
Wearing a mask for more than a few minutes causes a significant reduction in a person’s blood oxygen level.
- Beder, A., U. Büyükkoçak, H. Sabuncuoğlu, Z. A. Keskil, and S. Keskil. 2008. “Preliminary Report on Surgical Mask Induced Deoxygenation during Major Surgery.” Neurocirugia 19 (2): 121–26. DOI: 10.1016/s1130-1473(08)70235-5
- This study of 53 surgeons evaluated the effect of surgical masks on oxygen saturation of hemoglobin in surgeons performing surgery.
- The study revealed the surgeons experienced a significant decrease in the oxygen saturation of arterial pulsations (SpO2) and a slight increase in pulse rates after one hour. The decrease was more prominent in the surgeons over the age of 35.
- Given that a small decrease in SpO2 reflects a large decrease in partial pressure of oxygen in the arterial blood (PaO2)[R], the findings of this study suggests that surgical masks worn more than one hour may lower arterial oxygen enough to induce physiologically detrimental effects.
- Here are two cases of the tragic consequences of forcing children to wear masks: Two Chinese boys drop dead while wearing face masks during physical exercise classes.[R][R]Two boys from two Chinese cities died of sudden cardiac arrest within a week. The first boy, 15, collapsed after jogging in PE class while wearing a face mask on April 24. The other boy, 14, reportedly died during a running exam while wearing a mask.Why would healthy boys drop dead while wearing masks and running in gym class?! To answer this question, we must consider how mask induced deoxygenation and increased oxygen demands of heart muscle during exercise could have precipitated heart attacks in otherwise healthy teenagers:
- Point #1: Heart muscle needs oxygen to survive. And the harder the heart works, the more oxygen it requires. The American Heart Association says this about heart attacks:
- “Your heart muscle needs oxygen to survive. A heart attack occurs when the blood flow that brings oxygen to the heart muscle is severely reduced or cut off completely.”[R]
- Point #2: Masks block air intake and decrease arterial oxygen.
Studies of masked individuals have shown that mask wear decreases arterial oxygen. For example, the effects of surgical masks worn by surgeons in the operating room (an environment in which the oxygen blocking effects of masks are minimized by the high air flow, increased oxygen levels, and cool temperature of the operating suite) during major surgery showed a significant decrease in arterial oxygen.[R]
The lesson here is that medical masks should not be worn during intense exercise. As described above and shown in the study of surgeons wearing surgical masks, medical masks block oxygen intake. Depriving the heart of oxygen while exercising, especially intense exercise, could precipitate an acute heart attack.
Any questions? Wait…there’s more…
- Jogger’s lung collapses after he ran for 2.5 miles while wearing a face mask [R]Mr Zhang’s left lung was punctured due to high pressure caused by running. The 26-year-old became breathless whiling jogging with a mask on in China. Doctors said his punctured lung was caused by jogging with a face covering. He is now in stable condition after undergoing an operation, the hospital said.
- Hypoxia increases the risk of blood clot formation.[R]
- Lowering arterial oxygen suppresses the immune system, thus increasing the susceptibility of mask wearers to infectious disease.
3. Medical masks raise carbon dioxide levels in the blood.
Although the body has robust mechanisms for mitigating transient and minor elevations of CO2 in the air we breathe, these mechanisms can easily be overwhelmed by chronic exposure to significant elevations in CO2, such as occurs with prolonged wearing of a medical mask.
- The science clearly demonstrates that face masks cause carbon dioxide rebreathing and hypercapnia [R]
- Fletcher, S. J., M. Clark, and P. J. Stanley. 2006. “Carbon Dioxide Re-Breathing with Close Fitting Face Respirator Masks.” Anaesthesia 61 (9): 910. https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2044.2006.04767.x
- Exhaled air is rich in carbon dioxide, a waste product of cellular respiration.
- A portion of carbon dioxide previously exhaled is inspired (breathed) at each respiratory cycle.
- Masks trap CO2 rich respiratory exhalations at the mask-mouth interface, force re-breathing of CO2 rich exhalations, raise carbon dioxide blood (CO2) levels. [R]

- Objective evidence demonstrating how masks increase blood carbon dioxide levels and negatively impact health and function.
- Transcranial Ultrasound Doppler (TCUD) is a noninvasive means of assessing blood flow in the cerebral vasculature. The increase in carbon dioxide partial pressures (PCO2) caused by medical masks can be assessed by TCUD.[R]
- Elevation of PCO2 causes vasodilation of the arteriolar channels leading to a decrease in peripheral vascular resistance. The decrease in peripheral vascular resistance is responsible for the changes in cerebrovascular circulation time, CBF, and the velocity of flow (V) in cerebral arteries.
- Medical masks force the wearer to inspire (re-breathe) air that is a mix of air from the local environment and the respiratory waste products from the mask wearer’s previous exhalations.
- Respiratory exhalations contain significantly higher levels of carbon dioxide (CO2), one of the waste products of respiration.
- The pulmonary system is designed to collect oxygen and remove CO2 from the body. Masks trap CO2 rich exhalations at the mask-mouth interface.
- Changes in arterial PCO2 considerably influence cranial blood flow (CBF).[R]
- Transcranial Ultrasound Doppler (TCUD) studies on masked and unmasked individuals demonstrate the changes in blood flow in the brain the result from the arterial CO2 elevation that occurs within seconds of donning a mask.This video demonstrates the use of TCUD and heart rate variability to measure the adverse effects of masking a healthy nine year old child: https://bit.ly/2GGQWiZ
4. SARS CoV-2 is armed with a “furin cleavage site” that makes it more pathogenic.
- The furin cleavage site makes the virus more capable of invading human cells.
- The furin cleavage site makes the virus even more capable of invading cells when arterial oxygen levels decline.[R]
- Therefore, wearing a medical mask may increase the severity of CoVID-19.
5. Medical masks trap exhaled viral (and other) pathogens in the mouth/mask interspace, increase viral/infectious load, and increase the severity of disease.
- Face masks trap exhaled viral particles in the mouth/mask interspace. The trapped viral particles are prevented from removal from the airways. The mask wearer is then forced to re-breathe the viral particles, thus increasing infectious viral particles in the airways and lungs.
- In this way, surgical masks cause self-inoculation, increase viral load, and increase the severity of disease.
- Neurosurgeon, Russell Blaylock, MD, raises additional concerns:“By wearing a mask, the exhaled viruses will not be able to escape and will concentrate in the nasal passages, enter the lungs, olfactory nerves, and travel into the brain.”[R]
- Face masks trap exhaled viral particles in the mouth/mask interspace.[R] The trapped viral particles are prevented from removal from the airways. The mask wearer is thus forced to re-breathe the viral particles, increasing infectious viral particles in the airways and lungs. In this way, Medical masks cause self-inoculation, increase viral load, and increase the severity of disease.
- Asymptomatic or mild cases of CoVID-19 become more severe when the infected is masked, oxygen lowers, viral load increases from particle re-breathing, and the disease overwhelms the innate immune system.
- The main purpose of the innate immune response is to immediately prevent the spread and movement of foreign pathogens throughout the body.[R]
- The innate immune system plays a crucial role in destroying the virus, preventing infection, or decreasing the viral load to decrease the severity of infection.
- The innate immunity’s effectiveness is highly dependent on the viral load. If face masks increase viral particle re-breathing at the same time they create a humid habitat where SARS-CoV-2 remains actively infectious, the mask increases the viral load and can overwhelm the innate immune system.
- This trapping, re-breathing, and increasing pathogen load delivered to the lungs becomes dramatically more dangerous when the medical mask becomes contaminated with the opportunistic viruses, bacteria, and fungi that can grow in the warm, moist environment of the mask.
- “By wearing a mask, the exhaled viruses will not be able to escape and will concentrate in the nasal passages, enter the olfactory nerves and travel into the brain.” – Russell Blaylock, MD
6. SARS CoV-2 Becomes More Dangerous When Blood Oxygen Levels Decline
- Arterial oxygen desaturation is a critical issue in CoVID-19. The virus’ ability to infect cells is markedly enhanced by oxygen desaturation, which has been shown to occur even in the ideal operating room environment in which surgeons operate: high air flow/exchange systems, cool temperature, and higher room oxygen levels. when wearing a surgical mask.[R]
- One of the features that make SARS CoV-2 uniquely infectious is the “furin” sequence in the virus that activates increased ACE2 receptor attack and cellular invasion in low oxygen environments.[R]
7. The furin cleavage site of SARS CoV-2 increases cellular invasion, especially during hypoxia (low blood oxygen levels)[R]
- The furin cleavage site found in SARS CoV-2 is the likely result of the bioengineering “gain of function” (which means increasing the virulence of a pathogen) research conducted at the Wuhan Institute of Virology. This unethical, dangerous, and illegal-in-most-countries research is alleged to have been funded by Dr. Anthony Fauci (with $7.4 million taxpayer dollars) and Bill Gates.
- Furin cleavage sites are found in some of the most pathogenic forms of influenza, which can be acted upon by furin and other cellular proteases. The ubiquitous expression of cellular proteases across cell types increases the potential for the virus to successfully infiltrate the host.
- Furin is a membrane-bound protease that is expressed in multiple tissues throughout the human body. Furin is expressed in significant concentrations in the lungs. Thus, viruses in the respiratory tract can make use of this enzyme to convert and activate their own surface glycoproteins. This makes their role in viral protein processing noteworthy.[R]
- Some of the most pathogenic forms of influenza and HIV have similar furin cleavage sites. It is not present in other bat beta coronaviruses. (By the way, Fauci built his career researching and failing to create a vaccine for HIV). The furin cleavage site is NOT present in SARS CoV-1 or MERS, or any of the other known “bat coronaviruses.”
- Let me say it again, the SARS-CoV (aka, SARS-CoV-1), which is closely related to the newest SARS-CoV-2 strain, does not bear the furin cleavage site.
So, the question we should all be asking is how did the genetic sequence that codes for this serious gain of function that increases the potential for the virus to successfully infiltrate the host find its way into SARS-CoV-2?
That’s the trillion dollar question; it demands a real and honest answer.
8. Cloth masks may increase the risk of contracting Covid-19 and other respiratory infections.
See MacIntyre CR, Seale H, Dung TC, et al., A cluster randomised trial of cloth masks compared with medical masks in healthcare workers, BMJ Open 2015; 5: e006577, US National Library of Medicine, National Institutes of Health, doi: 10.1136/bmjopen-2014-006577, April 22, 2015. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4420971/pdf/bmjopen-2014-006577.pdf
- “This study is the first [Randomly Controlled Trial] of cloth masks, and the results caution against the use of cloth masks.
- This is an important finding to inform occupational health and safety. Moisture retention, reuse of cloth masks and poor filtration may result in increased risk of infection.”
9. Wearing a face mask may give a false sense of security
- People adopt a reduction in compliance with other infection control measures, including social distancing and hands washing.[R]
10. Masks compromise communications and reduce social distancing
- The quality and volume of speech between two people wearing masks is considerably compromised and they may unconsciously move closer to improve communications
- This increases the likelihood of becoming exposed to the infectious viral particles in the respiratory plumes of aerosolized droplet nuclei that escape the top, bottom, and sides of the masks.
11, Untrained and inappropriate management of face masks:
- The public is untrained and inadequately educated in the proper selection of masks (most are wrongly wearing cloth masks), proper wear, sterility management, and importance of not reusing single use masks.
- People must not touch their masks, must change their single-use masks frequently or wash them regularly, dispose of them correctly and adopt other management measures, otherwise their risks and those of others may increase.[R][R]
- We can all observe the countless ways in which people in communities are mis-wearing, mishandling, and increasing their own and the communities risk of contracting infectious disease, including CoVID-19.
12. Masks Worn Imperfectly Are Dangerous
To fully appreciate the danger of improper wear and handling of face masks, all you have to do is observe how the public is managing them. Take a trip to Walmart or your local school and observe how mask wearers pull masks from their pocket or purse, drop the masks on the floor, cough and sneeze in them, move them below the nose, on their heads, or under their chin. I see it every day. I also see their soiled and stained surgical face masks and know that these people are dangerously reusing a mask that should never be reused.
You don’t need a clinical trial to determine that even when mask-wearers manage to don a fresh, sterile mask properly, keep them on for more than a few minutes at a time, they very quickly contaminate the mask, their environment, and increase their risk of infection as the mask induces them to compulsively touch their faces and their masks.
- The World Health Organization, which has repeatedly changed its position on universal masking, is adamant that if face masks are not worn carefully, correctly, and kept sanitary, they are worse than ineffective.
- In other words, masks worn imperfectly are dangerous.
- See Linda Lacina, WHO updates guidance on masks for health workers and the public – here’s what you need to know, World Economic Forum (June 5, 2020). https://www.weforum.org/agenda/2020/06/who-updates-guidance-on-masks-heres-what-to-know-now/
People can infect themselves if they use contaminated hands to adjust a mask or repeatedly take it on or off,” explained WHO Director-General, Dr Tedros Adhanom Ghebreyesus. “I cannot say this clearly enough. Masks alone will not protect you from COVID-19.”
Failing to follow strict medical standards for wearing protective equipment and specification of sterilizing and cleaning often leads to “skin and mucous membrane injury, which may cause acute and chronic dermatitis, secondary infection and aggravation of underlying skin diseases.”
- Yan, et al., Consensus of Chinese Experts on Protection of Skin and Mucous Membrane Barrier for Health-Care Workers Fighting against Coronavirus Disease 2019. Dermatologic Therapy, March 2020, e13310. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7228211/pdf/DTH-9999-e13310.pd
13. Masks collect and colonize viruses, bacteria, and mold.
In Germany, where schools are open and masks are mostly optional, the association of “Kinder f.Weltfrieden eV” commissioned a laboratory analysis to investigate the level of microbial contamination that results after a fresh mask is worn by a child for 6-8 hours in school. What they found was alarming to all those recommending we mask our children for several hours every day. The masks were found to be contaminated with 82 bacterial colonies and 4 mold colonies. Where do you think the bacteria, molds, and viruses progressively colonizing and growing on the warm moist mask-mouth interface end up?
Many of the microbes get transferred to surfaces the child (or adult) touches after they touch, fiddle, and mishandle their mask. This is one of the many reasons that masks are almost certainly INCREASING the transmission of infectious disease. More dangerously, these microbes are being inhaled and delivered deep into the lungs where respiratory disease far worse than CoVID-19 can result.
The oxygen lowering effects of masks forces the body to compensate by increasing heart rate and deepening inspirations (increasing tidal volumes). Increased tidal volumes drives the mask pathogens deep into the lungs where they can cause serious pneumonia, inflammation, and tissue damage.
Furthermore, these risks are compounded by the immune suppression (CD4+ T-cell suppression) that results from diminished arterial oxygenation. Thus, the mask-wearing child is at imminent risk for harm caused by lung infections that are far more dangerous than a CoVID-19 infection.
In fact, based on reports from my colleagues in emergency medicine, pulmonology, and infectious disease, an alarming explosion in bacterial pneumonias is being reported at ERs and urgent care centers across the country.
Evidence that supports the points above:
- Zhiqing, Liu, Chang Yongyun, Chu Wenxiang, Yan Mengning, Mao Yuanqing, Zhu Zhenan, Wu Haishan, et al. 2018. “Surgical Masks as Source of Bacterial Contamination during Operative Procedures.” Journal of Orthopaedic Translation 14 (July): 57–62.
- This study investigated whether surgical masks (SMs) could be a potential source of bacterial shedding leading to an increased risk of surgical site infection.
- Results: The longer the operating time the more bacterial colonization occurred. A significant increase [in bacterial counts] was noted in the 2-hour group.
- Colleen Huber, NMD, “Masks Are Neither Effective nor Safe,” PrimaryDoctor.Org, July 6, 2020. https://www.primarydoctor.org/masks-not-effect
- “The foregoing data show that masks serve more as instruments of obstruction of normal breathing, rather than as effective barriers to pathogens. Therefore, masks should not be used by the general public, either by adults or children, and their limitations as prophylaxis against pathogens should also be considered in medical settings.”
- Dr. Huber’s article cites 42 supporting scientific studies.
- “Dr. Jenny Harries, England’s deputy chief medical officer, has warned that it was not a good idea for the public to wear face masks as the virus can get trapped in the material and causes infection when the wearer breathes in.”
- Angela Betsaida B. Laguipo, BSN, “Reusing Masks May Increase Your Risk of Coronavirus Infection, Expert Says,” News, Medical, Life Sciences, March 15, 2020. https://www.news-medical.net/news/20200315/Reusing-masks-may-increase-your-risk-of-coronavirus-infection-expert-says.aspx
- See also, Melkorka Licea, “Mask Mouth” Is a Seriously Stinky Side Effect of Wearing Masks. New York Post, August 5, 2020. https://nypost.com/2020/08/05/mask-mouth-is-a-seriously-stinky-side-effect-of-wearing-masks/
- Consider this: Health department investigating after high number of strep throat cases reported at Shepherd schools.The Central Michigan District Health Department is investigating after more than a dozen cases of strep throat were reported within Shepherd Public Schools despite COVID-19 protocols.
14. Wearing a face mask makes the exhaled air (respiratory plumes) go into the eyes.
- Masks may capture respiratory jets and large respiratory droplets, but they cannot prevent the respiratory plumes composed of aerosolizable respiratory droplet nuclei to escape the top, bottom, and sides of the masks.
- The respiratory plume wafts into the eyes and generates an uncomfortable feeling and compulsion to touch and rub the eyes. If your hands are contaminated and you touch or rub your eyes, you are transmitting and infecting yourself through the ocular mucosa.[R]
15. Contact tracing studies show that asymptomatic carrier transmission is very rare.
- Asymptomatic carriers are not a major driver of the disease.[R]
- Therefore, one of the key reasons the public was told to wear masks, asymptomatic spreaders, should not be used as a reason for community wearing of masks.
16. Face masks and stay at home orders prevent the development of herd immunity.
- Only herd immunity can prevent pandemics; it is the only thing that ever has.
- Only herd immunity will protect the vulnerable members of society.
- Sweden’s example continues to prove this point.
17. Face masks are dangerous and contraindicated for a large number of people with pre-existing medical conditions and disabilities.
- Large percentages of the population have medical conditions that make wearing a mask dangerous. Individuals should be examined by a medical professional to ensure that mask wear will not further compromise their medical condition.
- Children with asthma (7.5% of American children) and other respiratory disabilities are being harmed by mask mandates, they are being discriminated against by businesses, schools, and public spaces that require masks.
- Children with autism and other neurodevelopmental disorders are extremely prone to agitation and severe anxiety that results from the adverse effects, e.g., oxygen lowering effects, of masks.
- An ever increasing number of children and young adults with autism are sensitive to touch and texture.[R] Covering the nose and mouth with fabric can cause sensory overload, feelings of panic, and extreme anxiety.
- If a person with a disability is not able to wear a face mask, state and local government agencies and private businesses must consider reasonable modifications to a face mask policy so that the person with the disability can participate in, or benefit from, the programs offered or goods and services that are provided. A reasonable modification means changing policies, practices, and procedures, if needed, to provide goods, services, facilities, privileges, advantages, or accommodations to an individual with a disability.
- Examples of a person with a disability who might not be able to wear a face mask include individuals with asthma, chronic obstructive pulmonary disease (COPD), or other respiratory disabilities may not be able to wear a face mask because of difficulty in or impaired breathing. People with respiratory disabilities should consult their own medical professional for advice about using face masks.
- The CDC also states that anyone who has trouble breathing should not wear a face mask.[R]
- People with post-traumatic stress disorder (PTSD), severe anxiety, or claustrophobia (an abnormal fear of being in enclosed or narrow places), may feel afraid or terrified when wearing a face mask. These individuals may not be able to stay calm or function when wearing a face mask.
- A person who has cerebral palsy may have difficulty moving the small muscles in the hands, wrists, or fingers. Due to their limited mobility, they may not be able to tie the strings or put the elastic loops of a face mask over the ears. This means that the individual may not be able to put on or remove a face mask without assistance.
- A person who uses mouth control devices such as a sip and puff to operate a wheelchair or assistive technology, or uses their mouth or tongue to use assistive ventilators will be unable to wear a mask.
Masking School Children is Ineffective, Unnecessary, and Harmful
Face masks are not only ineffective, they are more dangerous than parents are being told. Scientific study after scientific study over the course of many years have concluded that wearing face masks for extended periods of time puts the wearer, especially children, in imminent risk of physical and psychological harms.
If the previous section (“Masks are Harmful”) did not serve to make you question much of what you have heard about the risks of medical masks, let us now examine what the science and experts say about masking children.
Mandatory masks in school are a ‘major threat’ to children’s development, doctors warn
Wednesday, 09 September 2020
The face mask requirement at school is bad for children’s general well-being and should be abolished, 70 doctors wrote in an open letter to Flemish Education Minister Ben Weyts.
The doctors want [Flemish Education Minister] Weyts to immediately reverse his approach: no face mask requirement at school, only protect the at-risk group and only advise people with a possible risk profile to consult their doctor.
“In recent months, the general well-being of children and young people has come under severe pressure,” the letter’s authors said. “We see in our practices an increasing number of children and young people with complaints due to the rules of conduct that have been imposed on them.”
The doctors mentioned anxiety and sleep problems as well as behavioural disorders and germaphobia, which is a pathological fear of germs. They are also seeing an increase in domestic violence, isolation and deprivation.
“Mandatory face masks in schools are a major threat to their development. It ignores the essential needs of the growing child. The well-being of children and young people is highly dependent on emotional attachment to others,” they wrote.
According to them, “the face mask requirement makes school a threatening and unsafe environment, where emotional closeness becomes difficult.”
Moreover, “there is no large-scale evidence that wearing face masks in a non-professional environment has any positive effect on the spread of viruses, let alone on general health. Nor is there any legal basis for implementing this requirement.”
“Meanwhile, it is clear that healthy children living through Covid-19 heal without complications as standard and that they subsequently contribute to the protection of their fellow human beings by increasing group immunity”.
“The only sensible measure to prevent serious illness and mortality caused by Covid-19 is to isolate individual teachers and individual children at increased risk,” they said.
“This risk assessment is not the task of the Ministry of Education,” the doctors underlined, “but the task of the treating physicians in consultation with their patients.”
– From The Brussels Times
The Great Barrington Declaration
A letter authored by 3 top epidemiologists and professors on October 4 th, 2020, has, as of 6:00 pm, October 9th, 2020, been signed by 4,051 Medical & Public Health Scientists and 7,247 Medical Practitioners. This is a portion of their consensus declaration:
“As infectious disease epidemiologists and public health scientists we have grave concerns about the damaging physical and mental health impacts of the prevailing COVID-19 policies, and recommend an approach we call Focused Protection.”
Thus, “The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk. We call this Focused Protection.”
Read the letter in full: https://gbdeclaration.org/
Forcing Children to Wear Face Masks is Unnecessary
Forcing children to wear face masks in school is ineffective, harmful, and unnecessary. The risk of CoVID-19 in children is so low (see, “Masks are Unnecessary” above) that any imagined benefits cannot possibly outweigh the risks. Based on CDC data, the risk of children between the ages of zero and 19 years of age dying from CoVID-19 is an incredibly low risk of 0.00195%. This rate is much lower than the risk of children dying from influenza.
In fact, there is a large and growing body of physicians, pediatricians, scientists, epidemiologists, and researchers around the world that are speaking out against the anti-scientific public health recommendations that have been forced upon the public and our children.[R] Those of us that have read the science have concluded that it is senseless and dangerous to force children to wear face masks in school:
- See e.g., Michelle Science MD, MSc, FRCPC, et. al., COVID-19: Guidance for School Reopening, Division of Infectious Diseases, The Hospital for Sick Children (“Sick Kids”), University of Toronto, Canada. https://www.sickkids.ca/PDFs/About-SickKids/81407-COVID19-Recommendations-for-School Reopening-SickKids.pdf
- The use of [Non-Medical Masks (“NMMs”)] in the school setting should be driven by local epidemiology with age-specific considerations.
- When transmission in the community is low, the use of NMMs throughout the entire school day should not be mandatory for elementary, middle or high school students returning to school.
- Safe masking practices (e.g. proper wearing/storage/removal) should be reinforced with educational materials provided to parents, students and teachers.
- Given the current epidemiology, the use of NMMs is not recommended for elementary school students.
- A Covid-19 cross-country study by the University of East Anglia in England found that a mask requirement was of no benefit and could even increase the risk of infection.
- Hunter, et al., Impact of non-pharmaceutical interventions against COVID- 9 in Europe: a quasi-experimental study, May 6, 2020. https://doi.org/10.1101/2020.05.01.20088260
- “We found that closure of education facilities, prohibiting mass gatherings and closure of some non-essential businesses were associated with reduced incidence whereas stay at home orders, closure of all non-businesses and requiring the wearing of face masks or coverings in public was not associated with any independent additional impact.”
Forcing Children to Wear Face Masks for Long Periods Risks Causing Them Physical Injuries.
The topic of the physical harms caused by masks was covered previously, but it is worth repeating a few of the key points:
Wearing a mask for more than a few minutes causes a significant reduction in a person’s blood oxygen level.
- See A. Beder, et al., Preliminary report on surgical mask induced deoxygenation during major surgery, Neurocirugía (2008). http://scielo.isciii.es/pdf/neuro/v19n2/3.pdf
- Transcranial Ultrasound Doppler (TCUD) studies on masked and unmasked individuals demonstrate the changes in blood flow in the brain the result from the arterial CO2 elevation that occurs within seconds of donning a mask.This video demonstrates the use of TCUD and heart rate variability to measure the adverse effects of masking a healthy nine year old child: https://bit.ly/2GGQWiZ
Wearing masks for extended periods increased incidences of headaches and negatively affected work performance.
- See Jonathan J.Y. Ong, et al., Headaches Associated With Personal Protective Equipment – A Cross‐Sectional Study Among Frontline Healthcare Workers During COVID‐19, Headache, the Journal of Head and Face Pain (May 2020). https://headachejournal.onlinelibrary.wiley.com/doi/full/10.1111/head.13811
Most children wear cloth masks.
- See Brittany Dionne, How hard is it to find a medical grade face mask?, WBRC News, April 18, 2020. https://www.wbrc.com/2020/04/18/how-hard-is-it-find-medical-grade-face-mask/
But wearing a cloth mask may increase the risk of contracting Covid-19 and other respiratory infections.
- See MacIntyre CR, Seale H, Dung TC, et al., A cluster randomised trial of cloth masks compared with medical masks in healthcare workers, BMJ Open 2015; 5: e006577, US National Library of Medicine, National Institutes of Health, doi: 10.1136/bmjopen-2014-006577, April 22, 2015. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4420971/pdf/bmjopen-2014-006577.pdf
- “This study is the first [Randomly Controlled Trial] of cloth masks, and the results caution against the use of cloth masks.
- This is an important finding to inform occupational health and safety. Moisture retention, reuse of cloth masks and poor filtration may result in increased risk of infection.”
Forcing Children to Wear Face Masks for Long Periods Risks Causing Them Mental and Psychological Injuries
Children are at risk for psychological trauma in multiple ways by being forced to wear face masks all day long at school. Doctors from around the country warn of the dangers to children of wearing face masks all day.
- See e.g., Jeffrey I. Barke, M.D., Open the schools without politics, American Thinker, June 10, 2020. https://www.americanthinker.com/blog/2020/06/open_the_schools_without_politics.html
Mandatory face coverings on children is very harmful to the child: learning is inhibited; critical interactions among students and between student and teacher are fractured; and the face covering is counterproductive, as kids will naturally touch their faces, thereby contaminating their covering. This new normal that many are advocating may well lead to a spike in childhood behavior problems such as learning disabilities, anxiety disorders, and depression, to name a few.
- See also Kathleen M. Pike, PhD, Why a Mask is Not Just a Mask, Global Mental Health Programs, Columbia University, April 17, 2020. https://www.cugmhp.org/five-on-friday/why-a-mask-is-not-just-a-mask
Many young children burst into tears or recoil when someone wearing a mask approaches. It’s so common that some elementary schools prohibit masks at the school Halloween parade. One reason for this is that the development of facial recognition is relatively weak in young children. According to University of Toronto psychologist, Dr. Kang Lee, it is not until kids are about 14 years old that they reach adult skill levels in recognizing faces. Before then, kids tend to see individual facial features, rather than recognizing the person as a whole. By putting on masks, we take away information that makes it especially difficult for children to recognize others and read emotional signals, which is unsettling and disconcerting. These issues may be especially true for children with autism spectrum disorder, including Asperger’s syndrome, who tend to have particular difficulties reading non-verbal cues.
Dr. Alice Kuo, President of the Southern California chapter of the American Academy of Pediatrics issued a statement criticizing Los Angeles County school reopening guidelines that require children wear masks as “not realistic or even developmentally appropriate for children.” She explained that, “wearing masks throughout the day can hinder language and socio-emotional development, particularly for younger children.”
- Local Pediatricians Urge Collaborative Decision-Making About Reopening Schools, Southern California chapter of the American Academy of Pediatrics, June 2, 2020. http://aapca2.org/wp-content/uploads/2020/06/AAP-CA2-press-release-on-schools-re-opening 6-2-20-Rev.pdf
Some of the serious psychological harms to children caused by extended mask wearing are tied to lack of facial and emotional recognition.
- See Christiane Bormann-Kischkel, Face Recognition in Children, Eur Arch Psychiatr Neurol Sci (1986) 236: 17-20. https://link.springer.com/article/10.1007/BF00641052
The use of salient visual speech cues is hidden by masks making learning difficult for young children.
- Kaylah Lalondea and Rachael Frush Holta, Preschoolers Benefit From Visually Salient Speech Cues, Journal of Speech, Language, and Hearing Research, Vol. 58, 135–150, February 2015. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4712850/pdf/JSLHR-58-135.pdf
- see also Martin Wegrzyn , et al., Mapping the emotional face. How individual face parts contribute to successful emotion recognition, PLoS ONE 12(5): e0177239, May 11, 2017. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0177239
- Lawrence Brancazio et al., Use of visual information in speech perception: Evidence for a visual rate effect both with and without a McGurk effect, Perception & Psychophysics 2005, 67 (5), 759-769. https://pubmed.ncbi.nlm.nih.gov/16334050/
- Mustapha Skhiri, Visual Cues in Speech Perception, Department of Computer and Information Science, Linköping University, GSLT, LiTH 20001/3/02. http://www.speech.kth.se/~rolf/gslt_papers/MustaphaSkiri.pdf
Voices of teachers and other students muffled through face masks makes learning more difficult, especially for any child with a diagnosed or undiagnosed hearing impairment.
- See Amanda B. Silberer, PhD, et al., Importance of High Frequency Audibility on Speech Recognition With and Without Visual Cues in Listeners with Normal Hearing, Department of Communication Sciences and Disorders The University of Iowa, March 2014. https://haar.lab.uiowa.edu/sites/haar.lab.uiowa.edu/files/wysiwyg_uploads/silberer_bentler_wu_aas _2014.pdf
The Center for Disease Control (“CDC”) has made clear that “Schools are an important part of the infrastructure of communities and play a critical role in supporting the whole child, not just their academic achievement.”
- See Preparing K-12 School Administrators for a Safe Return to School in Fall 2020. Guidance from the CDC to school Districts. https://www.cdc.gov/coronavirus/2019-ncov/community/schools-childcare/prepare-safe return.html
- Nowhere in the guidance provided to local schools by the CDC is any information about compelling students to wear face masks. In fact, the CDC acknowledges that “[m]ore research and evaluation is needed on the implementation of mitigation strategies (e.g., social distancing, masks, hand hygiene, and use of cohorting) used in schools to determine which strategies are the most effective.” Id. at 5.
The lack of any such recommendation is understandable given that the great weight of scientific evidence shows unmistakably that wearing face masks for extended periods is harmful to people’s health, safety and emotional well-being, especially to young children.


Purtarea măştii e obicei păgîn osândit de Sfinții Părinți :
Canonul 62 Trulan:
…să nu puie asupra lor obraze (măşti)
de haz (comice), sau de batjocură (satirice) închipuind satiri, sau de
jale, (tragice), nici să nu se strige numele blestematului Dionisos,
când se strivesc strugurii în teascuri, nici turnând vinul în vase să nu
stârnească (provoace) râsul, făptuind cele ale rătăcirii diavoleşti,
sub chipul neştiinţei sau al deşertăciunii.
De aceea, cei care de acum înainte s-ar apuca sa facă ceva din cele
zise mai înainte, după ce au fost puşi în cunoştinţă, poruncim ca
aceştia, dacă ar fi clerici, să se caterisească, iar dacă ar fi laici, să se
afurisească.